





Patient's Perspective
‘Solving the Myth’
Is ‘remission’ all about calculating disease activity scores? Do we need more drugs in our armamentarium or work on improving compliance? How well do our patients understand their illnesses? Are they able to cope? Do doctors overprescribe? The answers have multiple layers, and are not easy. The first and only step to understand their perspectives better is to engage with them and understand their predicament. Often in a busy OPD, we get lost in counting the joints, particularly in a rheumatoid patient, and forget that the disease has effects beyond joints. About 10–58% of patients have compliance issues. This could be multifactorial, but an imperative reason is lack of disease perception. The enigma of cure still lures them. They are not aware of how long the disease would last. Is it short-lived? They are taken aback by the cyclical nature of the disease, because they are caught unawares. We need to educate them and address this paucity of knowledge about their disease. We need to help them get rid of their fear of the unknown. It is essential to learn about some of the common issues patients face before we move to specific issues. We should not miss the larger picture in an attempt to be too focused.
A lot of emphasis and efforts are being made to educate patients and involve them in decision-making. In fact, EULAR has come up with guidelines for better patient education (PE), participation and recommendations for training for health professionals in delivering PE across Europe. The concept of shared decision-making has become an indispensable part of management.
In order to understand them better, the Gujarat Rheumatology Association organized a patient welfare program entitled Gujarat Rheumatology Initiative for Patient Welfare (GRIP): a program by the people, for the people with GReat Immune Power.
The patient partners, support group representatives, and patients themselves took center stage. It was aimed at making it interactive and help patients understand the concepts of shared decision-making, better engagement, forming support groups, and patient partners. Before the event, a small survey was conducted to understand the beliefs of patients about their illness, concern and beliefs about medications using the self-administered Brief Illness Perception Questionnaire (Brief- IPQ) and Beliefs about Medicines Questionnaire (BMQ).
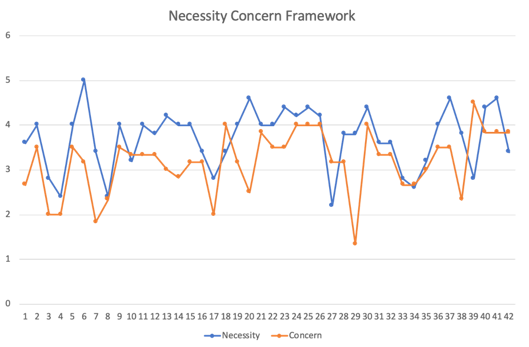
Figure 1: Beliefs about medication—Assessment of needs and concerns associated with the use of medications.
Figure 1 highlights the difference between the need for a particular medication for their disease (necessity) and concern about potential adverse consequences of using immunosuppressive drugs. Most patients rated necessity beliefs higher than concerns, which indicates positive views about disease-modifying drugs. But this might not be the true reflection, as the data were limited. The computed overall score derived from the Brief-IPQ was high, suggesting a more threatening view of the illness. Was this a driving force? This needs a more detailed evaluation to comprehend various components that make IPQ.
The program started with an introduction on autoimmune diseases. An insight into disease pathogenesis helped them to understand the burning question, why and how does the disease occur? Why me? This was followed by a demonstration of a typical journey of a patient in India and issues with wrong signposting. The biggest challenge is the improvement of patient–doctor engagement and equal participation of patients in delivering better care. An interactive session with the panelists helped in clearing myths surrounding these diseases and addressing a few questions such as:
a) Can it be cured? A tricky question, but the concept of remission was discussed. The control of disease with available medications and physiotherapy was discussed. A need for more awareness and disease education with early diagnosis and management was highlighted, as it will improve the chances of taking a patient close to ‘cure.’
b) The importance of a balanced diet and weight was highlighted. There are no restrictions on diet, except for patients with gout, who need to cut down on alcohol, red meat, and processed food.
c) Is it contagious? No, it is not.
d) Other important issues sich as impact on pregnancy and future generations were discussed, and the significance of keeping the disease in control for six months before conception was emphasized.
e) The importance of family education was also stressed.
Patients drew inspiration from each other’s stories, as the platform also allowed patients to detail their journey in their own words. A few queries from one patient were answered by another, thus encouraging discussion and better patient–patient engagement.
Patient support groups and leaders further highlighted how important it is for patients to be active in decision-making. They highlighted the concept of patient partners and the need for support groups. This will help them deal with issues on their own and work toward better solutions. The functionality and difficulties of patient support groups were touched upon, and patients were encouraged to be part of these.
The program ended with feedback from patients with a plan to conduct a three-monthly meet, moving from a general overview to disease-based themes. This was an effort of the Rheumatology Association of Gujarat (RAG) and involved Sjogrens’ India and Antardhwani (ankylosing spondylitis) as patient support groups.
The Indian Rheumatology Association has created a patient welfare cell, and a team is working on building educational material and videos for patients that can be used across the country with gradual availability of these in regional languages. The success of any such program largely depends on active patient participation. The long-term aim is to increase awareness about the disease at the national level and improve the typical journey of a patient. It is time to move hand in hand with the aim of ensuring a better patient–doctor and patient–patient relationship, as patients and professionals both bring different skills, values, and experiences to research and care.

Avinash Jain, MD, DM (SGPGI, Lucknow)

Bad Sleep and Bad Disease!
In our busy clinic, when a patient comes to us with many symptoms, we tend to neglect a few symptoms. One such symptom is lack of sleep. It is not uncommon to see patients with highly active rheumatoid arthritis complaining of insomnia. It is indeed perplexing when someone asks, “Why do we need sleep?” Recent research is beginning to answer this question. Much evidence shows that sleep is critical for proper memory, mood, performance, and health. Inadequate or disturbed sleep can result in accidents, reduced work productivity, stress, difficulty in relationships, and impaired health, which impact individuals, relationships, and society in general.Inflammation is often increased or unbalanced in individuals with sleep-related disorders, including insomnia, sleep apnea, and restless legs syndrome. Individuals who have diseases that tend to increase inflammation such as cancer, cardiovascular disease, stroke, type 2 diabetes, schizophrenia, Alzheimer’s disease, and autoimmune disorders, are more likely to have disturbed sleep. The increased prevalence of sleep disorders in old age is due to increased inflammation in old age.
Many proinflammatory cytokines such as IL-1 beta and TNF-alpha regulate sleep, health, and physiological functions, such as cognition, mood, performance, and fatigue, that are affected by sleep loss and disease. These proinflammatory cytokines are enhanced in the brain with sleep loss and are elevated in the brain at times of the day when one sleeps more.
Now it is evident that sleep is involved in the development of immunological memory; but additionally, there are data that suggest that sleep is important for other inflammatory homeostatic functions, as well.
Newer to the arena of the immune system and inflammatory research is the investigation of chronic inflammation, or the activation of inflammatory systems that fail to resolve completely. The following studies on sleep loss and the rise of inflammatory cytokines will give us more knowledge about the impact of sleep loss on inflammation.
1. Men who were permitted to sleep only two hours twice a day, once at night and once in the afternoon, for four days showed no increase in IL-6, TNF-alpha, or TNF-alpha receptors.
2. In another study that investigated the effects of ten days of sleep reduced to four hours per night, no change was found in TNF-alpha or its soluble type I receptor, although IL-6 was increased.
3. In another study, two hours of sleep reduction per night for seven nights led to increased TNF-alpha in healthy men but not women, but increased IL-6 in both men and women.
4. In a study of sleep restricted to four hours per night and centered on the mid-sleep time of habitual sleep, IL-6 and CRP were also found to be elevated.
5. Another recent study provided sleep opportunity for four hours/night for five nights and found increased IL-1beta, IL-6, IL-17, and hsCRP.
Sleep deprivation can lead to both micro and macrovascular reactivity changes preceded by increasing blood pressure, norepinephrine, and IL-6. Sleep loss can lead to insulin resistance and impaired glucose tolerance. An overnight sleep study in which cytokines and acute-phase proteins were measured showed that for each hour of reduced sleep obtained by polysomnography, there was 12% more circulating hsCRP and TNF-alpha and 9% more IL-6 in the fasting blood sample.
Patients experiencing chronic pain frequently were found to have elevated inflammatory mediators and impaired sleep. Inflammatory markers, including prostaglandins and proinflammatory cytokines, have been shown to sensitize nociceptors (i.e. decreasing their response threshold), thereby contributing to the development and/or amplification of spontaneous pain and hyperalgesia. Future research should focus on the role of inflammatory markers in sleep loss and pain. This will give us insights into the management of chronic pain syndromes.
Controlling the disease and ensuring patients get good sleep both go hand in hand in the treatment of inflammatory diseases. Hence to get better results, it is reasonable to consider managing sleep disorders associated with inflammatory diseases.
References
1.Mullington JM, Simpson NS, Meier-Ewert HK, Haack M. Sleep loss and inflammation. Best Pract Res Clin Endocrinol Metab. 2010;24(5):775-84.

Dr. P.S. Arul Rajamurugan, MD, DM
Assistant Professor of Rheumatology, Madurai Medical College,
Consultant Rheumatologist-Madurai Arthritis and Rheumatism Centre, Madurai, TN